
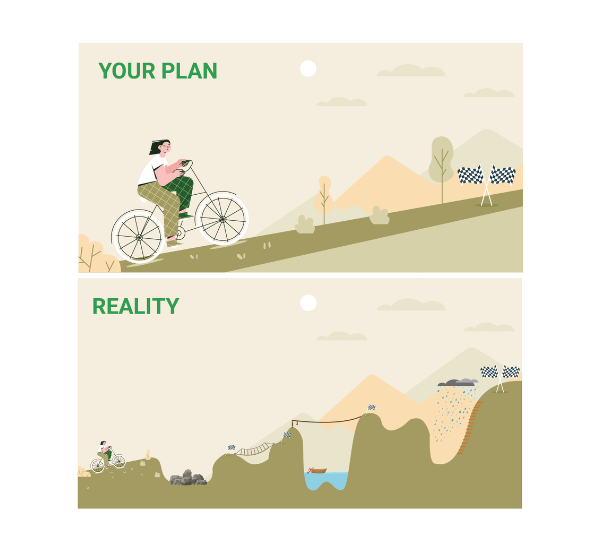
As you move through your rehab journey, there will be challenges along the way. You might remember this image from Module 5: What does recovery look like?
Going through rehab is very similar to driving on an uphill road. You might be expecting a smooth and steady drive to the top. But along the way, you notice that the road goes up and down. It can stay flat for a long time followed by sudden twists and sharp turns. The ride might be fun for some parts and boring at others. You might want to turn around and go home at some points. Then eventually you reach your destination.
Many drivers find it helpful to look at a map before going on a trip. This helps them to prepare for any difficult sections over rough terrain. Having realistic expectations of the road ahead can help you to keep going through the difficult moments.
This module will help you to understand some of the challenges you might face through rehab – and give you some tips and tricks to work through these difficult moments.
Most people find that their attention is worse after brain injury. This happens for people with mild, moderate and severe TBI (1). You might have trouble with one or more types of attention including visual (i.e. taking in imagery and objects around you), spatial (i.e. directing your attention to a location in space), or auditory (i.e. taking in important sounds and filtering out background noise).
Many people find it hard to do their rehab exercises when they have poor attention. Attention problems often cause feelings of frustration and hopelessness during rehab (2). You might want to give up because it feels like there’s there is no point in doing rehab – this is really common for people with TBI.
Doing as much as you can counts for a lot – whether it’s 10 seconds, 1 minute or 10 minutes. Each time you do an exercise, your brain creates new structures and pathways to replace the ones damaged during your injury. Over time, with practice and training, many people with a TBI are able to improve their attention (2).
It’s common for people with TBI to report new symptoms or difficulties months or years after injury (3). These new symptoms or difficulties which appear at a later time are called late effects or delayed effects (4). It can be scary when new symptoms suddenly appear. Some people think this means their TBI is getting worse – but this isn’t true. Late or delayed symptoms are caused by changes in the brain which occurred at the time of injury – they just take a long time to become noticeable (4).
It can be frustrating or discouraging to have to deal with new or changing symptoms. You might feel like you’re going backwards or starting again with your rehab whenever a new symptom appears. It’s important to recognise that this is a normal part of brain injury recovery (3).
It’s important to report any new symptoms to your rehab team as soon as you notice them. Your team will be able to modify your rehab exercises and help you work on any new areas.
Fatigue is very common after TBI. It’s estimated that around 80% of people with a TBI have problems with fatigue which can last for as many as five years after injury (5).
Normal fatigue is a conscious decrease in a person’s ability to perform physical or mental tasks or activities (6). It’s often described as a feeling of physical or mental weariness that occurs after a period of activity or exertion (7).
For example, you might feel physically fatigued after a few rounds of strength and conditioning exercises with your physio. This is caused by muscle exertion. Or you might feel mentally fatigued after doing some communication exercises with your speech therapist. You can feel physically and mentally fatigued at the same time.
With a TBI, you will find that you become fatigued faster and more easily after doing activities (7). Let your therapists know whenever you need a break.
Sometimes you may feel fatigued even if you have not done any activities, and the fatigue may not disappear after rest. This is called pathological fatigue and is caused by changes in the brain and body after injury (7). This type of fatigue is more intense and prolonged than normal fatigue (8), can be difficult to treat and can interfere with your rehab.
Sometimes, fatigue and low energy levels can be caused by sleep problems. Over 50% of people with a TBI experience some form of sleep disturbance (9). There are behavioural treatments or medications to help with sleep problems. Your rehab team can liaise with your doctor to prescribe any medications if needed.
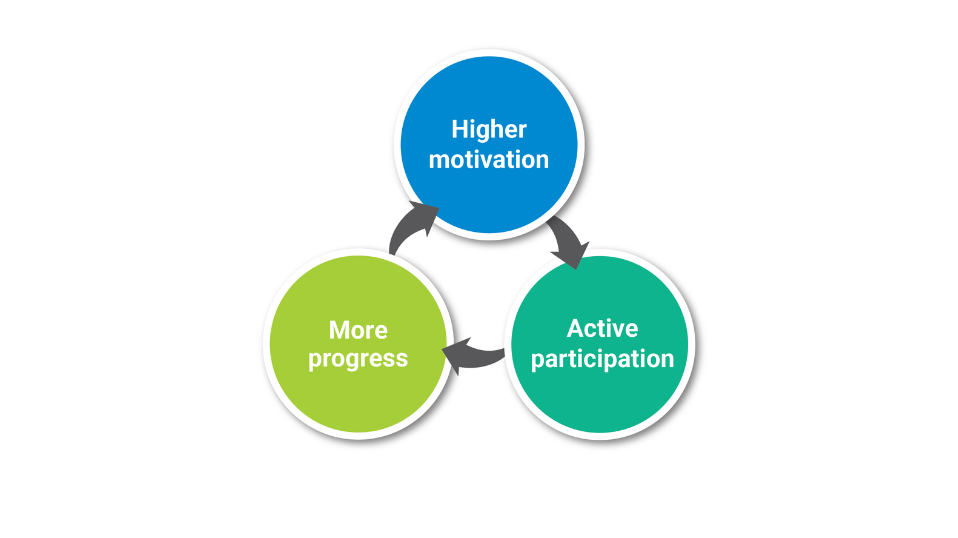
Motivation is important in determining the outcome of rehabilitation (10). Generally, people who have higher motivation show larger improvements at the end of rehab compared to those with lower motivation (11). Researchers believe this happens as people who have higher motivation are more likely to actively participate (or try their best) in rehab. They are then more likely to make progress – which in turn boosts their motivation (12). This is called a positive feedback loop (13).
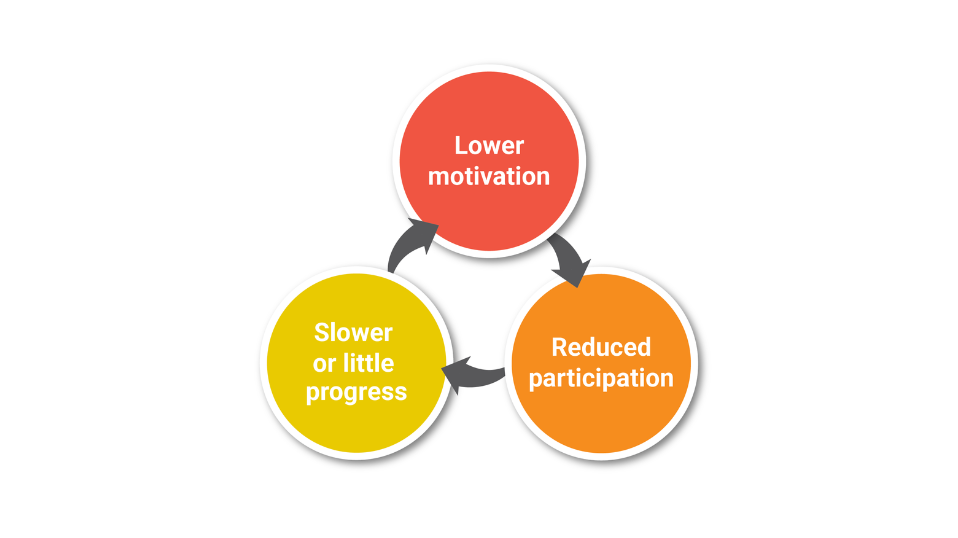
The opposite happens when a person has low motivation. People with lower motivation are less likely to try their best during rehab. This causes them to show slower or little progress – which in turn reduces their motivation. This is called a negative feedback loop. So as you can see, motivation is really important.
But it’s not realistic to be highly motivated throughout your whole rehab journey. Most people find that their motivation goes up and down. This is normal.
When you’re feeling unmotivated, the trick is to try not to stay in the low motivation zone for too long – or you might get stuck in the negative feedback loop.
Here are some ways to increase your motivation when you’re just not feeling it:
There may be other challenges that come your way during rehab. A typical rehab program can take 1-2 years to complete so there can be lots of changes that happen along the way. Some possible challenges include:
Your rehabilitation coordinator or case coordinator will be an important person throughout your rehab journey. They will communicate with you about any changes to your team, services or funding.
It’s also important for you to communicate with your rehabilitation coordinator if you’re having any issues with any part of your program, team or peers. They will be able to support you to find